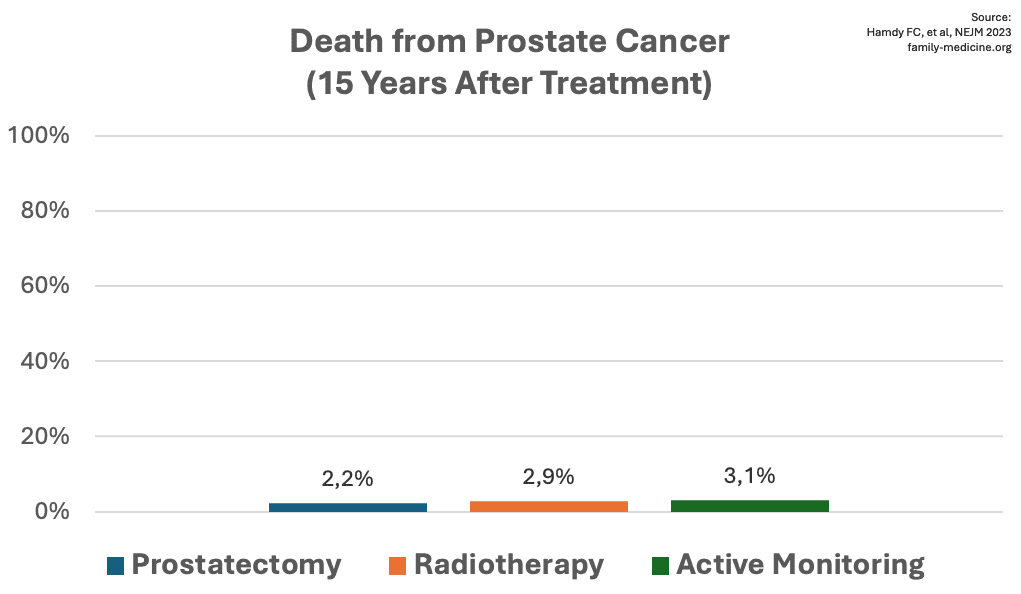
Published in the NEJM in 2023, this RCT recruited 1,643 patients from the UK aged 50-69 with localized prostate cancer. They received either prostatectomy, radiotherapy or active monitoring. Of course, patients could change treatment later (61% of those under active monitoring did so). After a median follow-up of 15 years, 356 men died, thereof “only” 45 from prostate cancer (13% of deaths). There was no significant difference (P=0.53) concerning death from prostate cancer between the three treatment options:
Other outcomes were significantly worse for active monitoring vs. prostatectomy/radiotherapy. Specifically, metastases developed in 9% vs. 5%, androgen deprivation therapy was initiated in 13% vs. 7%, and clinical progression occurred in 26% vs. 11%.
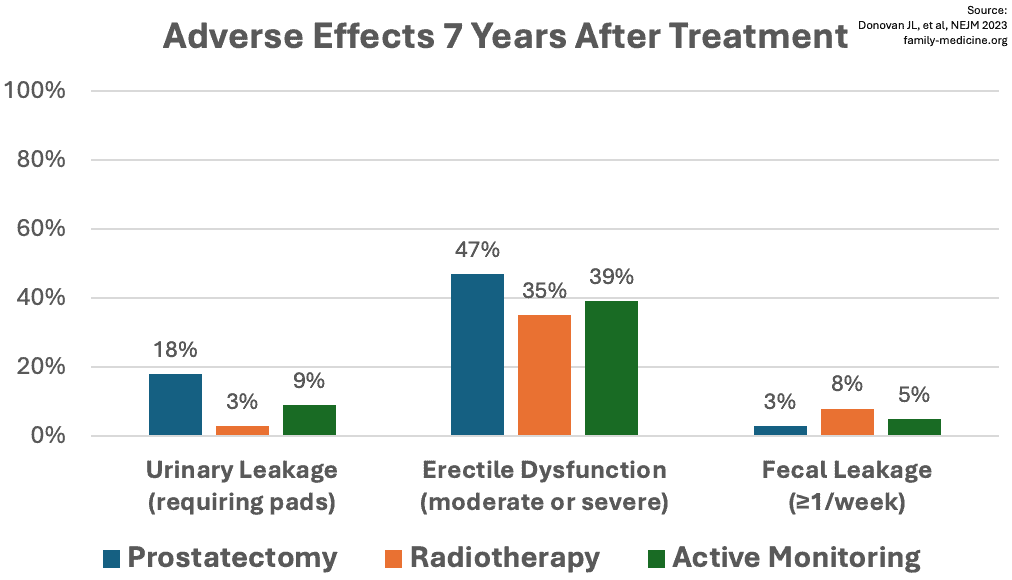
However, patient-reported outcomes were worse for radical prostatectomy, namely long-term urinary and sexual harms:
The study authors concluded that “patients newly diagnosed with localized prostate cancer should carefully consider the trade-offs between treatment harms and the risks of prostate cancer progression in the context of low cancer-specific mortality”.